EUP 🇪🇬
6.6K subscribers
About EUP 🇪🇬
Egyptian union of pediatricians
Similar Channels

Gian Domenico Caiazza
Rappels quotidiens autour du Tawhid

UNIÓN DE ESTANQUEROS

Panchamrut Dairy (Amul)

Unión Estudiantil - FCA

๋ʬ ּPLOWSIE ✮ helpeu 100%

Jyotiraditya M. Scindia

CSIF Lugo

AIUBOSA (AIBOA)
Mohamed Atef - محمد عاطف

Pabitra Margherita

💙 TuS Union Scharfenberg 🤍

USCI - Unione Statistica dei Comuni Italiani

Actu VTC - Union Indépendants

Planet Rugby
Swipe to see more
Posts
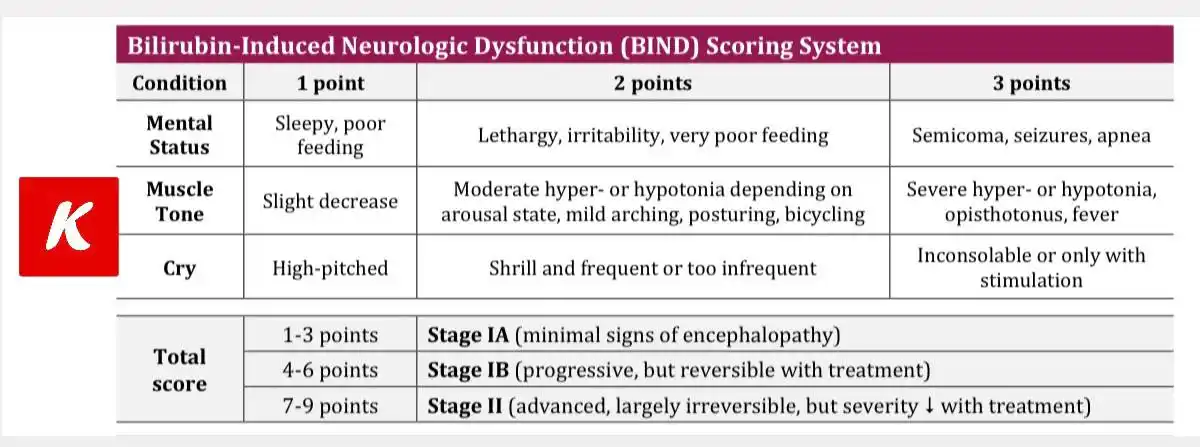
BIND Score – Used in jaundiced newborns to detect early signs of bilirubin toxicity and prevent kernicterus. It evaluates 3 key areas: 🧠 Mental status 💪 Muscle tone 🗣️ Cry pattern Each gets a score from 1 to 3 → total guides severity: ✅ Mild (1–3) ⚠️ Moderate (4–6) ❗ Severe (7–9) The higher the score, the higher the risk of neurologic damage. Early detection = timely treatment = better outcomes! #Neonatology #BINDscore #Jaundice #NICU #NewbornCare #KernicterusPrevention

ان شاء الله النهارده الجمعة ٢٠ يونيو في تمام الساعة السابعة مساء بتوقيت القاهرة *When* : Jun 20, 2025 07:00 PM Cairo *Topic* : Past, Present and Future In Neonatal Mechanical Ventilation Dr Tarek Kotb 🌍 #British_Wheel *#Link* Join from PC, Mac, iPad, or Android: https://us02web.zoom.us/j/81652242910 *Webinar ID:* 816 5224 2910
صباح الخير الزووم مفتوح الآن Developmental and Psychosocial Paediatrics Dr Nancy Mokhtar https://us02web.zoom.us/j/83097278426 @everyone
https://youtu.be/w-StNo3jfUw?si=COgGrGNIcZCzChDM *#اخترنا_لك*
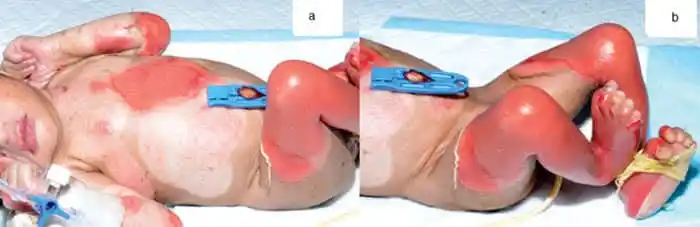
علي الرغم من كونها حالة طبية نادرة مرتبطة بالأمراض الجلدية إلا أنك كطبيب أطفال من المؤكد أنك ستقابلها علي الأقل مرة أو مرتين في الحياة العملية. إنها حالة انحلال البشرة الفقاعي أو Epidermolysis bullosa or EP. انحلال البشرة الفقاعي هي مجموعة من الحالات الجلدية الوراثية الجينية التي تورث بصفة جسدية سائدة أو متنحية علي حسب النوع. تم التعرف علي ما يقرب من ٣٠٠ طفرة جينية مسئولة عن مرض انحلال البشرة الفقاعي. العلامة المميزة لانحلال البشرة الفقاعي هو حدوث بثور Blisters وفقاعات Bullae في الجلد عند الولادة أو بعد الولادة بقليل مع هشاشة شديدة بالجلد. هذه البثور والفقاعات تحدث بصورة أكبر في الأماكن المعرضة للاحتكاك والخدش ولكن في بعض الأحيان قد تحدث تلقائيا. هذه البثور والفقاعات تختلف في توزيعها وشدتها حسب النوع فقد تشمل اليدين والقدمين فقط وقد تشمل الجلد كله والممرات التنفسية Respiratory airways والأغشية المخاطية Mucous membranes مثل الفم والمرئ والقناة الهضمية. بعض الحالات الخفيفة من الممكن أن تظهر في سن المراهقة أو مرحلة البلوغ ولكن معظم الحالات تظهر مع الولادة أو بعد الولادة بقليل أو حينما يبدأ الطفل في الحبو والزحف. كما ذكرنا فإن انحلال البشرة الفقاعي حالة وراثية جينية قد تحدث نتيجة انتقال جين واحد من أحد الوالدين المصاب بالمرض (وراثة جسدية سائدة Autosomal dominant) أو من كلا الوالدين (وراثة جسدية متنحية Autosomal recessive). لمعرفة أنواع ومكان حدوث كل نوع يجب معرفة أن الجلد يتكون من طبقة خارجية تسمي البشرة Epidermis تحتها طبقة تسمي الأدمة Dermis وبينهما الغشاء القاعدي Basement membrane. لذلك تنقسم حالات انحلال البشرة الفقاعي إلي ثلاث أنواع رئيسية علي حسب مكان حدوث البثور والفقاعات. كل نوع من هذه الأنواع الثلاث ينقسم إلي عدة أنواع أخري علي حسب الطفرة الجينية وتوزيع حدوث البثور والفقاعات. هذه الأنواع هي: ١) انحلال البشرة الفقاعي البسيط Epidermolysis bullosa simplex or EBS : يورث هذا النوع بطريقة جسدية سائدة Autosomal dominant. هذا النوع ينقسم إلي : * انحلال البشرة الفقاعي البسيط الموضعي Localized EBS أو ما يعرف سابقا بنوع فيبر كوكايين Weber Cockayne's type: أكثر الأنواع شيوعا وتحدث البثور والفقاعات في اليدين والقدمين وغالبا ما تظهر عندما يبدأ الطفل بالحبو ولا تترك ندبات بعد الالتئام ولكن يحدث خشونة في باطن اليد والقدم مع خشونة في الجلد. * انحلال البشرة الفقاعي البسيط العام Generalized EBS أو ما يعرف سابقا بنوع كوإيبنر Koebner's type : غالبا ما تشمل الجلد كله وبخاصة اليدين والقدمين والساقين. تحدث البثور والفقاعات عند الولادة أو بعد الولادة بقليل وقد تشمل الأغشية المخاطية والأظافر ويحدث أيضا خشونة في جلد باطن اليدين والقدمين. * انحلال البشرة الفقاعي البسيط العام الخطير أو Generalized severe EBS أو ما يعرف سابقا بنوع داولينج ميارا Dowling Meara's type: نوع خطير يظهر غالبا عند الولادة ويؤثر علي الجلد بصفة عامة والوجه والجذع وغالبا ما يشمل الأغشية المخاطية للفم والمريء والمجاري التنفسية والأظافر. قد يحدث تيبسات في المفاصل contractures مع صعوبة في الحركة. ٢) انحلال البشرة الفقاعي التواصلي Junctional epidermolysis bullosa or JEB : يورث بطريقة جسدية متنحية Autosomal recessive. تحدث البثور والفقاعات عند الغشاء القاعدي Basement membrane. ينقسم هذا النوع إلي : * انحلال البشرة الفقاعي التواصلي العام الخطير Generalized severe JEB أو ما يعرف سابقا بنوع هيرلتز Herlitz type: أشد أنواع هذا النوع خطورة ويظهر منذ الولادة ويشمل الجلد كله وقد يشمل الأعضاء الداخلية. قد يظهر عند الولادة بفقاعة واحدة وتزداد في العدد تدريجيا حتي تشمل الجلد كله. بحة الصوت مع السعال Hoarseness of voice with cough قد تكون علامة لتأثر الممرات التنفسية. قد تحدث مضاعفات خطيرة مثل العدوي infection وسوء التغذية malnutrition والجفاف dehydration وحالات كثيرة تموت في خلال العامين الأوائل بعد الولادة. * انحلال البشرة الفقاعي التواصلي العام المتوسط Generalized intermediate JEB أو ما يعرف سابقا بنوع الغير هيرلتز Non Herlitz type: غالبا ما يشمل فروة الرأس والأظافر و الأسنان ويظهر عند الولادة أو بعد الولادة بقليل. قد تحدث مضاعفات مثل العدوي وسوء التغذية والجفاف والتي قد تؤدي إلي الوفاة ولكن الحالات التي تعيش غالبا ما تتحسن بمرور الوقت. ٣) انحلال البشرة الفقاعي الحثلي Dystrophic epidermolysis bullosa or DEB : تحدث البثور والفقاعات في الجزء الأعلي من الأدمة وينقسم هذا النوع إلي : * انحلال البشرة الفقاعي الحثلي العام السائد Dominant generalized DEB: تحدث البثور والفقاعات عند الولادة وتشمل الجلد كله. مع نمو الطفل وبداية الحبو والمشي تتركز البثور والفقاعات علي اليدين والقدمين ومفصل الركبة والكوع. قد تتأثر أيضا الأغشية المخاطية بما فيها المريء. تترك البثور والفقاعات علامات بيضاء بعد الالتئام تعرف بال milia. هذا النوع قد يكون مصاحبا لضمور أو نقص خلقي في تكوين بعض مناطق الجلد Aplasia cutis congenita مع اعتلال بالأظافر Nail dystrophy فيما يعرف جميعا بمتلازمة بارت Bart's syndrome. * انحلال البشرة الفقاعي الحثلي العام المتنحي الخطير Generalized severe recessive DEP أو ما يعرف سابقا بنوع هالوبيو سيمنز Haloppeau Siemens type وانحلال البشرة الفقاعي الحثلي المتوسط Generalized intermediate DEP أو ما يعرف سابقا بنوع الغير هالوبيو سيمنز Non Haloppeau Siemens type: تظهر البثور والفقاعات علي سطح الجلد بالكامل عند الولادة والتي تكون خطيرة مع اشتمال الأغشية المخاطية والمريء ( النوع المتنحي الخطير أكثر شيوعا من النوع المتوسط). تحدث ندبات شديدة مع تيبسات والتصاقات بالأصابع فيما يعرف بال Mitten hands كما قد يحدث تضيق في المرئ Esophageal stricture مع حدوث سوء تغذية وجفاف وعدوي ثانوية قد تؤدي إلي الوفاة. قد يحدث سرطان الجلد الحرشفي Squamous cell carcinoma كأحد المضاعفات. كما ذكرنا يوجد العديد من الأنواع الأخري النادرة جدا تحت كل نوع من الأنواع الثلاث الرئيسية. مؤخرا تم إضافة نوع رابع يعرف بمتلازمة كيندلر Kindler's syndrome حيث تحدث البثور والفقاعات منذ الولادة مع حدوث حساسية للضوء Photosensitivity وقد تتأثر الأغشية المخاطية والعين و الأسنان. تحدث البثور علي القدمين واليدين تاركة تصبغات جلدية Hyperpigmentation مع مناطق ضمور بالجلد skin atrophy ومناطق أخري من الجلد الخشن Keratosis. يتم تشخيص حالات انحلال البشرة الفقاعي عن طريق الصورة السريرية المميزة Clinical picture. تكون ظاهرة كوإيبنر Koebner's phenomenon موجبة في حالات انحلال البشرة الفقاعي (ظهور البثور والفقاعات في أماكن الجلد الطبيعي عند حدوث احتكاك بها) كما تكون علامة نيكوليسكي Nikolsky sign موجبة (احتكاك الجلد المجاور للبثور والفقاعات يؤدي إلي انفصال طبقات الجلد بعضها عن بعض). يتم أخذ عينة من الجلد Skin punch biopsy للتشخيص الأكيد وعمل التحليل الجيني Genetic test لمعرفة الطفرة الجينية المسببة للمرض وذلك للاستشارة الوراثية Genetic counseling. مرض انحلال البشرة الفقاعي مرض غير قابل للشفاء. العلاج يتكون من تفادي الخدش والاحتكاك مع ارتداء الملابس الناعمة التي تقلل من الاحتكاك بالجلد. نحتاج في كثير من الأحيان إلي استعمال المضادات الحيوية لحالات العدوي البكتيرية الثانوية 2ry bacterial infection مع استعمال غيار جراحي ناعم ومرطب باستمرار علي أماكن البثور والقرح. يجب أن تكون التغذية عالية السعرات الحرارية High caloric diet وقد نحتاج للتغذية الكاملة عن طريق الوريد Total parenteral nutrition في حالات سوء التغذية وضعف النمو. قد نحتاج أيضا إلي علاج فقر الدم الناتج عن سوء التغذية أو حدوث نزيف بالقناة الهضمية GIT haemorrhage وإمكانية نقل الدم Blood transfusion والذي يعتبر تحديا كبيرا في هذه الحالات حيث أن الوخز والاحتكاك يعتبر مسببا أساسيا لحدوث البثور والفقاعات. تضيق المرئ Esophageal stricture قد يحتاج إلي عملية بالمنظار لتوسيعه. التفريق التشخيصي لانحلال البشرة الفقاعي يشمل العديد من الحالات الأخري مثل مرض الفقاع Pemphigus والمرض الفقاعي المزمن في الأطفال Chronic bullous disease of childhood ومرض اعتلال الجلد الخطي الفقاعي المصاحب للجلوبيولين المناعي A أو linear IgaA bullous dermatosis (كل هذه الأمراض تعتبر من أمراض المناعة الذاتية Autoimmune diseases) والمرض الفقاعي الناتج كمضاعفات لأدوية معينة Pemphigoid drug reaction و انحلال الجلد الفقاعي المكتسب Epidemolysis bullosa acquisita ( أيضا أحد أمراض المناعة الذاتية ولذلك قد تستخدم أدوية تثبيط المناعة Immunosuppressive drugs في علاج هذا النوع). هناك أيضا القوباء الفقاعية Bullous impetigo الناتج عن التهاب بكتيري ببكتيريا المكورات العنقودية Staphylococci. أيضا هناك البثور الناتجة عن الاحتكاك Friction blisters ( في أماكن الاحتكاك مثل باطن اليد والقدم و الأصابع وتكون غير خطيرة وتلتئم في وقت قصير بلا أية مضاعفات). مرض البورفيريا Porphyria وهو مجموعة أمراض وراثية تحدث نتيجة لخلل في التمثيل الغذائي في تصنيع البورفيرين Porphyrin الضروري لتكوين الهيمجلوبين (تتميز مجموعة أمراض البورفيريا بالتقرحات والبثور التي تحدث غالبا عند التعرض للضوء مع حساسية الجلد للضوء وأعراض عصبية مثل التهاب الأعصاب الطرفية وألم بالبطن والعضلات والعظام مع تغيير في لون البول وأعراض هضمية وغيرها). أخيرا هناك متلازمة تحرق الجلد المصاحب للمكورات العنقودية Staphylococcal scalded skin syndrome ومتلازمة ستيفنس جونسون Stevens Johnson syndrome. العديد من هذه الحالات من الممكن تفريقها عن انحلال البشرة الفقاعي عن طريق أخذ تاريخ مرضي مفصل وتاريخ دوائي Drug history وتاريخ عائلي Family history والفحص السريري الشامل لمعرفة العلامات الأخري المصاحبة أو عن طريق عينة الجلد Skin biopsy. د/وليد علي إبراهيم المرواني. زميل الكلية الملكية لطب الأطفال.
موعدنا غدا إن شاء الله الجمعة 20 يونيو 8 صباحا بتوقيت القاهرة في بث مباشر استراليا و أول محاضرة من محاضرات طب الأطفال التطوري والسلوكي بعنوان 📌Basics of Developmental and Psychosocial Paediatrics تقدمها د نانسي الشيخ استشاري طب الأطفال – إدارة صحة الأطفال والمراهقين، ولاية غرب أستراليا زميل الكلية الملكية الأسترالية للأطباء – تخصص طب الأطفال وصحة الطفل عضو الكلية الملكية البريطانية لطب وصحة الطفل – المملكة المتحدة ماجستير طب كبد الأطفال – المعهد القومي للكبد، جامعة المنوفية بكالوريوس الطب والجراحة – جامعة المنوفية، مصر 📌 رابط الزوم https://us02web.zoom.us/j/83097278426